Healthcare Panic Buttons for Hospital Staff Safety: Complete Guide for 2026
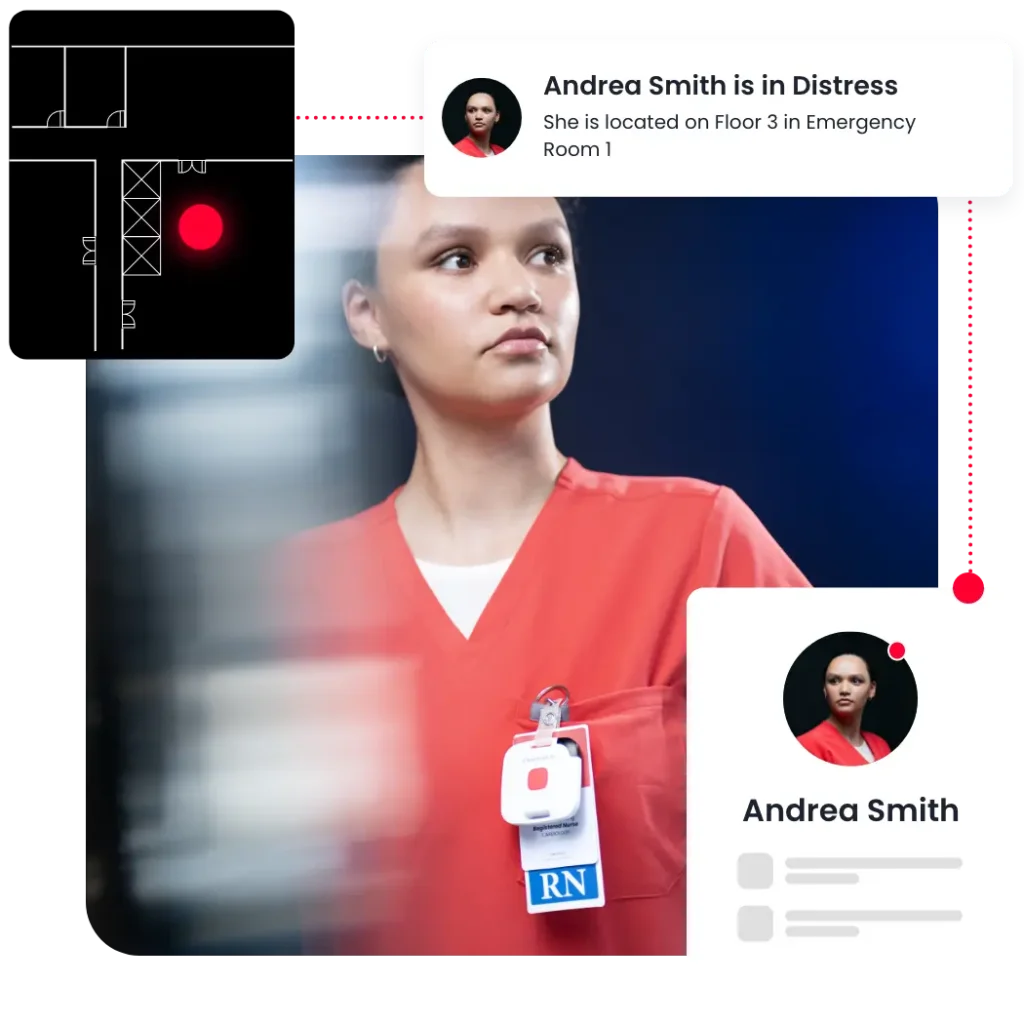
The emergency department charge nurse presses her badge. Security arrives 22 seconds later at the correct room, instead of standing around in the hallway or searching the floor above. Once they get there, they see the patient’s behavioral flags are already on screen, and ultimately, the interaction de-escalates before anyone gets hurt.
That sequence happens thousands of times a day across hundreds of hospitals, but only where panic button systems are treated as infrastructure, not accessories. The gap between those two approaches explains why on average, two nurses are assaulted every hour in the U.S. while only 22% of hospitals provide portable panic buttons.
How does a nurse panic button actually work?
A healthcare panic button is a wireless, wearable device that triggers location-specific alerts when pressed. Modern systems broadcast the wearer’s position through Bluetooth Low Energy (BLE) or Wi-Fi networks, sending alerts to security personnel, nearby staff, and designated responders within seconds. Rather than serving as a simple alarm, the button press activates a coordinated response sequence.
The technology relies on three components: the wearable badge with the button, a network of sensors or access points that track location, and software that routes alerts to the right responders. When a nurse presses the button (typically three rapid presses to prevent accidental activation), the system identifies who pressed it, where they are, and where the closest available responders are located. Response teams receive alerts via text, mobile app, desktop notification, or integrated nurse call systems.
What separates effective systems from inadequate ones is room-level location accuracy and response orchestration. Knowing a nurse needs help “somewhere on the third floor” wastes seconds that determine whether an incident escalates or resolves. Kontakt.io’s platform combines BLE for campus-wide coverage with selective infrared (IR) for room certainty, enabling alerts that identify the exact room, and not the general area.
What’s the difference between a nurse call button and a panic button?
Nurse call buttons are patient-activated devices that request routine assistance for clinical needs like medication, bathroom help, or meal service. Panic buttons are staff-activated emergency devices that summon immediate security or safety response for threatening situations. The technologies often integrate with each other, but serve distinct purposes with different response protocols and urgency levels.
Nurse call systems route requests through clinical workflows and prioritize based on acuity and staffing. Panic buttons bypass those workflows entirely, triggering immediate security responses regardless of other priorities. In hospitals with integrated platforms, both systems can share the same RTLS infrastructure and badge hardware, but the alert types, response teams, and escalation protocols differ completely.

Wearable vs. fixed panic buttons for healthcare: which is better?
Wearable panic buttons protect nurses wherever violence occurs; fixed buttons only protect staff within reach of a wall-mounted device. Since healthcare workers experience violence at a rate nearly five times higher than the private industry average, and incidents happen during patient transport, in hallways, break rooms, parking structures, and patient rooms, wearable systems provide substantially better coverage than fixed installations.
At hospitals where RTLS-based security devices were deployed, studies found that up to 80% of staff felt safer. The portability advantage compounds in multi-building campuses where nurses move between units, floors, and buildings throughout their shifts.
Fixed panic buttons made sense when wireless technology was unreliable and room-level location tracking was impossible, but that era is already over. Given their reliability, the real question for 2026 is which wearable system provides room-level accuracy, integrates with existing infrastructure, and supports other use cases beyond staff safety.

Can a hospital panic button locate the nurse who pressed it?
Yes, but only systems with room-level location accuracy deliver fast enough responses to prevent escalation. Knowing a distress call came from “Building 3” or “the fourth floor” leaves security guessing which room to enter and delays response by 30 to 90 seconds. Those seconds determine whether responders arrive before or after an assault.
Kontakt.io’s platform achieves room-level certainty through a hybrid approach: BLE provides campus-wide coverage and general location, while IR confirms the specific room. This combination delivers sub-three-second location-aware alerts with 100% room accuracy, enabling security to move directly to the correct entrance without searching hallways or checking multiple rooms.
Location precision matters for another reason: coordinated response. When the system knows exactly where the incident is occurring, it can identify the nearest appropriately trained responders, display relevant patient behavioral flags, and route backup resources without verbal coordination. That orchestration layer turns scattered responders into an organized team.
Do panic buttons integrate with existing nurse call systems?
Modern panic button platforms integrate with nurse call systems, electronic health records (EHRs), building management systems, and security infrastructure through open APIs and standard protocols. Integration enables richer context during incidents (patient behavioral history, sitter assignments, room occupancy) and eliminates duplicate infrastructure costs.
Kontakt.io’s platform connects with Epic, Cerner, Meditech, and other major EHR systems to surface relevant patient information when a duress alert triggers. It also integrates with leading nurse call systems including Rauland, Hill-Rom, and Ascom, allowing a single wearable badge to handle both routine nurse call cancellation and emergency duress alerts.
The integration question hospitals should ask is not “can it integrate” but “what does integration actually enable.” If connecting to the nurse call system only means displaying alerts on an additional screen, the value is minimal. If integration means the panic button system can pull patient behavioral flags, identify which responders are trained in de-escalation, and automatically log incident details for Joint Commission reporting, the value compounds.
What features should a healthcare panic button system have?
At minimum: room-level location accuracy, sub-five-second alert delivery, mobile and desktop alert distribution, responder acknowledgment tracking, and incident documentation for compliance reporting. Systems lacking any of these features create response gaps that increase injury rates and fail to meet regulatory requirements.
Beyond minimum features, effective systems provide response orchestration that routes alerts based on proximity, training, and availability. They surface patient context (behavioral flags, isolation status, sitter assignments) at the moment of need. They integrate with existing infrastructure rather than requiring parallel installations. They support campus-wide coverage including parking structures, ambulance bays, and courtyards, not just interior hallways.
Kontakt.io’s intelligent care operations platform adds predictive and agentic AI layers that identify indicators of increased violence risk and suggest workflow adjustments that reduce caregiver exposure. For example, the system can flag when a patient who has triggered multiple duress events in other hospitals is scheduled for admission and recommend additional de-escalation resources.
How do you train nurses to use panic buttons effectively?
Training requirements for modern panic button systems are minimal because the user interaction is simple: press the button three times rapidly when threatened. Most hospitals complete training in under five minutes during badge distribution, focusing on when to activate (at the first sign of escalation, not after violence occurs), how to press (three rapid presses), and what happens next (immediate alert to security and nearby trained responders).
The real training challenge is not teaching nurses how to press a button but creating a reporting culture where staff actually use the system when threatened. According to a 2024 American College of Emergency Physicians survey, 68% of healthcare workers felt their employer did not handle workplace violence reports appropriately, and 50% said nothing was done after reporting an incident. In environments where reporting is discouraged or ignored, underreporting persists regardless of technology quality.
Effective hospitals treat duress button activation as expected behavior, not a last resort. They communicate response protocols clearly: who responds, how quickly, what support follows. They track metrics like response time and incident closure rate, sharing data transparently to demonstrate the system works. They avoid penalizing staff for “false alarms,” recognizing that early activation during de-escalation is the correct response, not overreaction.
How do you reduce false alarms on nurse panic buttons?
False alarms drop to near zero when badges require three rapid presses rather than a single button push. This activation method prevents accidental triggers from bumping against doorframes, leaning over beds, or sitting down while still allowing genuine activation in under one second.
Kontakt.io’s Smart Badge 3 Mini vibrates when activated, providing tactile confirmation the alert was sent. This feedback mechanism reduces anxiety about whether help was actually summoned and eliminates repeated pressing that can create duplicate alerts.
The more significant challenge is defining “false alarm.” If a nurse activates the system during a tense interaction that then de-escalates before security arrives, that is not a false alarm, it is successful early intervention. Hospitals that penalize staff for activating “unnecessarily” train nurses to delay pressing the button until violence actually occurs, which defeats the purpose of early response systems.
Can panic buttons work through hospital walls and dead zones?
Modern BLE-based panic button systems achieve campus-wide coverage including through walls, stairwells, elevators, and traditional dead zones. The technology uses a mesh network of wall-mounted sensors (often called beacons or anchors) spaced throughout the facility, with each sensor covering a 50 to 150-foot radius, depending on construction materials and layout.
Dead zones occur in older installations using Wi-Fi-only tracking, which struggles with concrete walls, metal equipment, and elevator shafts. BLE signals penetrate these barriers more reliably and at lower infrastructure cost. For areas with particularly challenging RF environments, strategic sensor placement fills gaps.
Parking structures, courtyards, and outdoor walkways require deliberate coverage planning but are entirely feasible with modern systems. Kontakt.io’s platform provides the same protection in parking garages and ambulance bays as in patient care floors, because workplace violence follows nurses wherever they go, from shift changes at 11 PM to supply runs to offsite warehouses.
Which states require panic buttons for healthcare workers?
New York, New Jersey, California, Illinois, Washington, and Texas have enacted or are implementing laws requiring healthcare facilities to provide staff with immediate access to panic button systems or similar emergency response technology. In addition, over 60% of U.S. states have enacted or are actively pursuing workplace violence prevention mandates, with healthcare facilities facing specific obligations under various state laws.
New York’s law (signed in 2023) requires healthcare employers to provide “appropriate means of emergency notification” including panic buttons for at-risk staff. California’s SB 1299 (2014) mandated workplace violence prevention plans for hospitals, with panic button systems becoming the standard compliance method. Illinois HB 2396 (2024) requires hospitals to provide “effective means” for staff to summon assistance, with wearable panic buttons meeting the statute.
Regulatory compliance is the floor, not the ceiling. Hospitals must now determine what system actually keeps nurses safe and meets operational needs beyond simply checking a compliance box. Kontakt.io’s platform helps hospitals exceed regulatory requirements while supporting additional use cases like equipment tracking and patient flow optimization, that improve the return on infrastructure investment.
What’s the average response time for a hospital panic button?
Legacy fixed-button systems average 90 to 180 seconds from activation to responder arrival because security must locate the incident by following alarm sounds or radio dispatch. Modern wearable systems with room-level location accuracy achieve median response times under 30 seconds, with 90th percentile times under 45 seconds.
Kontakt.io customers report 60% reductions in response time compared to previous systems, with location-aware alerts delivered in under three seconds and 80% of events resolved before escalation. The improvement comes from eliminating the location search: when security knows exactly which room and which entrance, they move directly to the incident rather than searching floors.
Response time matters because de-escalation windows are narrow. A confrontation that escalates from verbal threats to physical assault typically takes 15 to 60 seconds. Response systems that cannot deliver trained responders within that window arrive after violence occurs, not before. The shift from “respond to violence” to “prevent escalation” requires response times measured in seconds, not minutes.
How much does a hospital-wide panic button system cost?
Cloud-based platforms like Kontakt.io’s reduce upfront infrastructure costs by leveraging existing BLE networks and eliminating on-premise server requirements.
The ROI calculation extends beyond badge costs. According to the American Hospital Association’s 2025 study, hospitals spent $18.27 billion managing workplace violence in 2023, a nearly seven-fold increase from $2.7 billion in 2016. Workplace violence incidents average $100,000 per injury incident when including treatment, workers’ compensation, temporary staffing, and regulatory reporting.
Across a 200-bed hospital, avoidable costs from violence-related incidents, staff turnover, and recruitment expenses total roughly $2 million annually. A panic button system that reduces violence frequency and severity by even 20% pays for itself within the first year.
Infrastructure sharing amplifies ROI. When the same RTLS deployment supports staff safety, nurse call cancellation, equipment tracking, and patient flow visibility, the per-use-case cost drops significantly. Kontakt.io’s platform enables this multi-purpose approach through an open architecture that adds capabilities without replacing infrastructure.
How long does it take to deploy a nurse panic button system?
Kontakt.io deploys staff safety infrastructure in as little as 2.5 working days for a 200-bed hospital. Installation averages six minutes per room (approximately 20 total hours) because the platform uses battery-powered sensors requiring no electrical wiring or Ethernet drops.
Cloud-native architecture eliminates the months-long deployment timelines associated with on-premise servers and custom integration work. From contract signature to live deployment in the first high-risk unit typically requires four to six weeks including infrastructure assessment, sensor placement, integration configuration, badge distribution, and staff training.
Phased rollouts enable hospitals to validate response protocols in emergency departments or behavioral health before expanding to full campus coverage. North Georgia Health System and Genesis HealthCare System both deployed campus-wide staff safety including parking structures and outpatient facilities within weeks rather than quarters.
For multi-hospital health systems, Kontakt.io deploys a single tenant with per-facility reporting, enabling one vendor relationship and one audit posture across the system rather than separate negotiations at each campus. This standardization cuts deployment time while improving data consistency for system-level safety analytics.
Training remains minimal regardless of facility size: three rapid presses when threatened. Most hospitals complete initial training in under five minutes during badge distribution.
Why room-level certainty matters more than general location
The difference between “third floor, west wing” and “Room 312” is whether security arrives before or after an assault. General location tracking narrows the search but still requires responders to check multiple rooms, listen for disturbances, or request additional information via radio. Room-level accuracy eliminates that search entirely.
Kontakt.io’s hybrid BLE-plus-IR approach achieves room certainty without requiring full IR coverage campus-wide. BLE handles general location and campus navigation; IR confirms the specific room when precision matters. This selective precision model balances cost, deployment complexity, and accuracy requirements.
The precision advantage compounds during incident response. When responders know the exact room, they can position appropriately (one to the door, another to bedside), review patient behavioral history before entering, and coordinate without verbal radio traffic that might escalate the situation. That orchestration layer turns location data into coordinated action.
Orchestration beats notification: why response coordination matters
A panic button that only says “help” externalizes all coordination work to stressed responders in the middle of a crisis. Modern systems should route alerts based on proximity, identify appropriately trained responders, surface patient context, and enable acknowledgment tracking so everyone knows who is responding.
This is the architectural shift defining staff safety in 2026: orchestration over notification. Kontakt.io’s platform routes duress alerts the way an experienced charge nurse mentally triages tasks, considering who is closest, who has de-escalation training, which staff are already managing other incidents, and what patient factors (behavioral flags, sitter status, isolation requirements) responders need to know.
For CNOs, this orchestration reduces the cognitive load nurses carry during every shift. When the system quietly coordinates responses, nurses spend less mental energy worrying about whether help will arrive and more energy delivering patient care. That reduction in hypervigilance and ambient stress directly addresses burnout drivers that fuel turnover.
For IT and Security Directors, orchestration means the safety platform integrates into the hospital’s operating layer rather than sitting as a standalone system. Duress events trigger coordinated workflows rather than isolated alerts, incident data feeds compliance reporting automatically, and the same infrastructure supports multiple use cases from asset tracking to patient flow.
What hospitals should expect from panic button vendors in 2026
Stop accepting systems that only provide location without response coordination. Demand room-level accuracy, not floor-level approximation. Require open APIs that integrate with existing infrastructure rather than proprietary silos.
Insist on cloud-native architectures that eliminate on-premise server maintenance. Expect multi-use platforms where staff safety is one capability among several, not a single-purpose gadget.
Ask vendors: what is your median response time, not your best case? How do you handle dead zones in parking structures? Can your badges support both staff safety and nurse call cancellation? Do you integrate with our EHR to surface patient behavioral flags? How do you orchestrate responses when multiple alerts trigger simultaneously?
The Kontakt.io platform answers those questions through an intelligent care operations platform that treats staff safety as part of hospital flow orchestration, not a separate system. The same RTLS backbone that tracks duress events also enables predictive patient flow, equipment visibility, and workflow optimization, spreading infrastructure costs across multiple high-impact use cases.